Basic Airway Delivery Tools and Care
Oropharyngeal Airway (OPA)
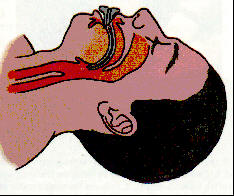
An oropharyngeal (OPA) airway is used to help establish a
patients airway when a is not present. OPA’s come in many sizes. To ensure proper size the
rescuer should measure by placing one end of the device on the corner of the
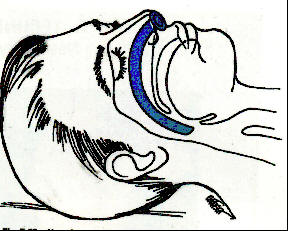
and the other end to the earlobe. To insert the OPA, hold the device
at its flange end and insert it into the mouth with the tip pointing toward
the roof of the patient’s mouth. Once the distal end of the OPA reaches the
posterior wall of the pharynx, rotate the OPA 180 degrees so that it is
positioned over the tongue. The flange should rest on the
when properly inserted. Use of the OPA does not eliminate the need
for maintaining proper head position.
 It is
also acceptable to rotate the device at 90 degrees.
It is
also acceptable to rotate the device at 90 degrees.
Nasopharyngeal Airway (NPA)
The NPA is used when the oral pharynx is not accessible or the patient has a gag reflex. The device is contraindicated in patients with and used with caution if are present. To ensure proper size the rescuer should measure from the corner of the to the earlobe. Lubricate the device prior to placement with a water based substance. When inserting the NPA in an emergency on should pick the largest and straightest nostril. Place the bevel of the NPA to the nasal septum. Hold the device like you would a pencil and slowly insert the NPA into the patient’s nostril until the flange is flush with the nostril. Do not force the device. Use of the OPA does not eliminate the need for maintaining proper head position.
Mouth-to-Mask and Bag-Valve-Mask
Mouth-to-mask breathing is the preferred method of ventilating a nonbreathing patient. It is a simple one person device, and because of the two-handed mask seal it provides excellent ventilatory volumes. The device when not connected to supplemental oxygen will deliver % oxygen to the patient. When attached to >10 LMP of supplemental oxygen the device delivers approximately % oxygen.

The bag-valve-mask (BVM) consists of a -way valve, -inflating bag, reservoir, and a mask. The device delivers % oxygen concentration with room air and once connected to high flow
supplemental oxygen it can deliver up to 80 to % oxygen concentration. The BVM technique commonly creates a poor
seal around the patient’s mouth and is designed for two trained rescuers to
use. The BVM typically delivers volume than mouth-to-mask technique. When using a BVM during a
cardiac arrest the rescuer needs to be aware of the pop-off valve status
because greater ventilatory pressure is usually required. This device is most
effective when the patient is intubated and the BVM is attached to an
endotracheal tube (ETT) because the trachea is then isolated.
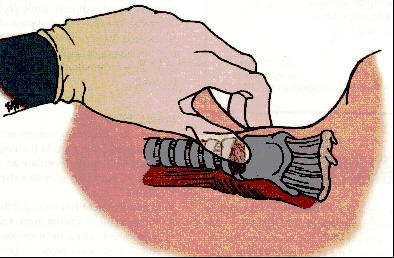
Sellick’s Maneuver (Cricoid Pressure)
Sellick’s maneuver reduces gastric inflation during ventilatory efforts. By placing downward pressure on the cartilage the diameter of the esophagus is decreased therefore restricting the flow of air into the stomach.
Suction
If a patient’s airway is compromised by fluids, turn the victim head to one side and remove large particles. Once suction is available the remaining fluids and fine particles should be removed. For oral suctioning the pressure should be set at approximately mmHg and suction limited to seconds. For tracheal suctioning the pressure should be around to 120mmHg and suction time limited to seconds. Only suction on the way out and always measure for proper advancement depth of the suction catheters.